Ein globales Netzwerk für Evidenz, Weiterbildung und biologisch-orientierte Zahnmedizin mit Fokus auf Keramikimplantaten
Mit großer Freude geben wir bekannt, dass die ISMI eine duale Mitgliedschaft mit der ICBI – International Circle for Biological Implantology eingegangen ist.Für alle ISMI-Mitglieder bedeutet das: Sie sind ab sofort auch Teil der ICBI, ohne Veränderung des Mitgliedsbeitrags im ersten Jahr – und profitieren damit von einem starken internationalen Netzwerk, hochwertigen Fortbildungsangeboten und dem Zugang zu führender wissenschaftlicher Expertise im Bereich der biologischen Implantologie
Was ist die ICBI?
Die ICBI ist eine wissenschaftlich orientierte, global agierende Organisation, die sich der Weiterentwicklung, Förderung und internationalen Verbreitung biologischer Implantologie verschrieben hat. Mit einem klaren Fokus auf biokompatible keramische Implantate verbindet die ICBI wissenschaftliche Tiefe mit klinischer Relevanz – und verfolgt dabei einen ganzheitlichen, patientenzentrierten Ansatz.
ICBI versteht sich nicht nur als akademische Plattform, sondern als Netzwerk die Zahnmedizin neu denkt – interdisziplinär, innovativ und international.
Die Vorteile Ihrer ICBI-Mitgliedschaft auf einen Blick:
🔬 Zugang zu wissenschaftlicher Evidenz
🎓 Exklusive Fortbildungsformate
🌍 Globales Netzwerk & Community-Effekt
Einblick: ICBI Consensus Conference – Evidenz trifft Gemeinschaft
Ein besonderes Highlight der ICBI-Aktivitäten ist die im September 2025 erstmals stattfindende ICBI Consensus Conference in Nizza. Dort kommen international unabhängige führende Expert:innen zusammen, um auf Basis aktueller Daten klinische Standards für den Einsatz von Keramikimplantaten zu definieren – ein transparenter, strukturierter und partizipativer Entscheidungsprozess, der der gesamten Community zugutekommt.
ISMI & ICBI – eine starke Partnerschaft
Die Verbindung von ISMI und ICBI bedeutet für alle Mitglieder einen bedeutenden Schritt in Richtung integrierter Wissensvermittlung, stärkerer Internationalisierung und eines lebendigen fachlichen Austauschs.
Sie behalten alle ISMI-Vorteile – und gewinnen mit der ICBI eine neue, internationale Dimension hinzu.
Der Mitgliedsbeitrag bleibt im ersten Jahr unverändert – und wir laden Sie herzlich ein, diese Gelegenheit zu nutzen, sich aktiv einzubringen, mitzuwachsen und mitzugestalten.
Mehr zur ICBI:
🌐 www.icbi.org
Willkommen in der Zukunft der biologischen Zahnmedizin. Willkommen bei ICBI.
by Dr Dominik Nischwitz
At present, ceramic implants (Fig. 1) are routinely used by only a few dentists: This is also evident in the small number of scientific studies compared to titanium implants. Therefore, the empirical facts resulting from the practical use of ceramic implants are particularly more important at this stage. The benefits of ceramic implants with regard to its biocompatibility, soft tissue reaction and the aesthetic result are now undisputed.
Ceramic implants react differently to conventional titanium implants. This poses the requirement to learn to “think in ceramic”. In this context, both the nature and biology of the body as well as the basic principles of immunology and biochemistry as well as bone and tissue regeneration are very important. Unlike titanium implants, ceramic implants only heal in absolutely healthy bone. The body recognises them as neutral and osseointegrates them during the bone regeneration phase. By comparison, titanium implants heal by means of inflammatory activation. Local inflammatory mediators remain constantly active depending on how prone the patient is to inflammation (high/low responder). To successfully insert ceramic implants, there are important basic rules to follow.
Systemic preparation for the operation (obligatory)
The Bone Healing Protocol (BHP® according to Dr Dominik Nischwitz) has proven effective for the perioperative support of bone regeneration and is used ahead of all surgical procedures to support the body’s own regeneration. At least 14 days prior the planned operation, it is crucial that the nutrients are consumed precisely according to this protocol. Poor nutrition with too much sugar, wheat and cow’s milk products as well as a lack of sunlight depletes the body of important vitamins and minerals: mainly vitamin D3 (lack of sun), zinc, magnesium and omega-3 fatty acids. This deficiency frequently causes the body to become overwhelmed with healing processes—it is almost in a state of “hibernation” and is not able to build new tissue as the nutrients to do so are simply not there.
Therefore, the patient’s diet, at least at this stage, should be as hypoallergenic and nutritious as possible. Common nutritional allergies and all compromising food additives are to be strictly avoided so that the immune system can concentrate on its most important task of constructing bone- and soft-tissue. A gluten and cow’s milk-free diet is recommended. Alcohol, tobacco and caffeine should be kept to a minimum and sugar, sweeteners, flavor enhancers, trans fats and other compromising food ingredients and additives should be completely avoided. Proteins, healthy fats and vegetables should be consumed. It is also important for the patient to drink plenty of fluids (daily consumption of 2 to 3 litres of still water).
Bone quality
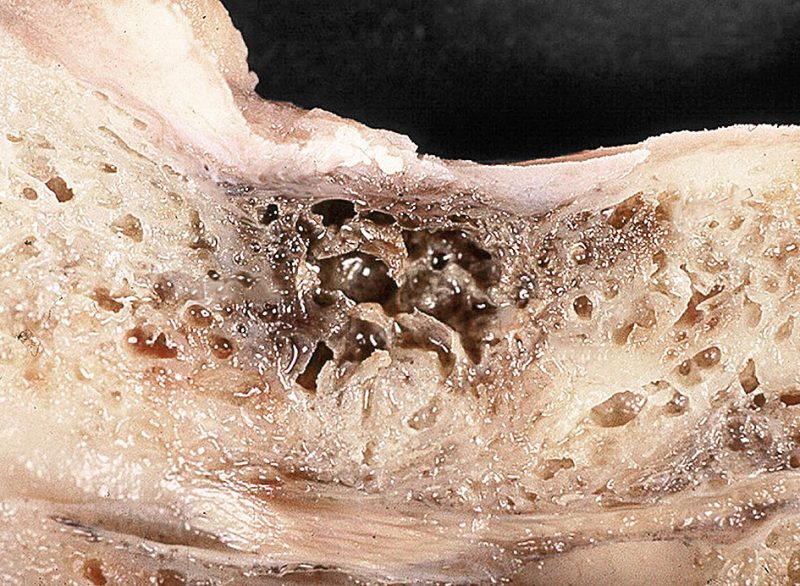
According to university doctrine, there are four bone density categories that classify the ratio of mineralised bone substance to bone volume. As our experience has shown, bones classified as category 3 and especially 4 are defective or even diseased (Fig. 2).
Every implantologist knows the phenomenon of “falling” into cavities while drilling. Chronic inflammations in the jaw bone frequently occur as result of wounds caused by tooth extractions in the past, which have not healed properly, tooth development or foreign particles. These inflammations are often not visible on conventional X-ray images. Similar to root-treated teeth, inflammatory mediators (TNF-, IL-1, RANTES) can also cause symptoms in other parts of the body. Neurological (NICO) or joint problems frequently occur. NICO stands for “neuralgia-inducing cavitational osteonecrosis”, which refers to chronically inflamed areas in the jaw bone. This osteolysis is also referred to as ischemic necrosis, a typical interference field in the jaw, which is also included in the category of neuromodulative triggers. Ceramic implants do not heal in bones of category 3 or 4. For this reason, osteolysis needs to be treated before implantation can occur. The bone must be absolutely healthy to ensure a successful implant healing (Fig. 3). The development of osteolysis is caused by a lack of nutrients as stated above.
Disinfection and plasma membrane
These osteolytic areas of bone contain fat cysts, degenerated trabeculae and allow chronic infections, particularly anaerobes, to feel at home in this area, triggered by the ischemic change in the bone. According to studies conducted by Lechner, increased heavy metals and other environmental toxins become deposited here. This bone area must therefore be cleaned and disinfected during implantation with the utmost precision.
Conditions for ideal bone healing:
The bone must be hard. There must be no “yellow bone”. The blood must be clear (no drops of grease or “foamy” blood).
In addition to implant drilling, piezosurgery has proven to be successful in order to remove diseased bone.
Osteolysis frequently affects the N. alveolaris inferior or the upper jaw up to the sinuses—the piezoelectric technique allows the dentist to carry out procedures even in critical areas, since due to the use of rotating instruments soft tissue injuries are unlikely to occur.
For disinfection we recommend ozone (Fig. 4). Ozone is a proven bactericide, virucide and fungicide. It therefore kills all microorganisms present. This facilitates healing as the immune system does not need to deal with additional infections. The use of ozone is indicated particularly after root-treated teeth have been extracted and ceramic implants have been immediately inserted (SCC® Short Cut Concept according to Dr Karl Ulrich Volz). In addition to the ozone production, the voltage formed in the glass vial (OzoneDTA; Fig. 5) stimulates bleeding.
Plasma (A-PRF™, PRGF®, etc.): In the author’s practice, inserting a plasma membrane (PRGF® or Choukroun A-PRF™; Fig. 6) gained from the patient’s own blood has proven to be effective. The blood is freshly extracted from the patient’s vein, centrifuged for around eight minutes and then activated (PRGF®). After 15 to 30 minutes, the membrane is ready for insertion. The plasma membrane technology is 100 per cent autologous and therefore completely biocompatible.
Combined with ozone therapy, plasma membrane insertion is a key part of all surgical procedures in our practice and is used after tooth extraction, in implants, for bone formation and as an insert following NICO removal. When using endogenic membranes, the regeneration of bone- and soft-tissue is phenomenal.
The whole protocol should be followed before and after every tooth extraction and must be followed for every surgical procedure on the bone. Thanks to this procedure, dry alveoli belong to the past.
Neural therapy and infusions
To further support the body’s own regeneration, the alveolus is rinsed with procaine after disinfection and then infiltrated with Traumeel in the vestibulum. Procaine is an anti-inflammatory local anaesthetic that stimulates blood circulation at the site. This ensures clean bleeding following the vasoconstringent of the anaesthetic. Furthermore, additional medication can be used: Notakehl (homeopathic antibiotic), Selenium (orthomolecular antibiotic) and Arthrokehlan “A” (“antitoxin”).During larger operations, such as a sinus lift, infusions are used on a routine basis: The combination of “single shot” antibiotics and cortisone (dexamethasone) has proven effective even at the operation day. The positive properties of antibiotics are used—which are basically prevention of infection—without the side effects caused by the oral intake (e.g. increased stress on liver and intestine).
Furthermore, the immune system is supported by a high dose of vitamin infusions administered intravenously as part of the surgical and ozone treatments.
Properties of ceramic implants
In addition to the numerous benefits of ceramic implants compared to titanium implants, there are also certain special features and even disadvantages. For example, ceramic implants do not dissipate heat. During the operation, it is thus extremely important for the surgeon to use the bone properties at the site for orientation. Unlike titanium implants, ceramic implants should be inserted with regard to the bone categories. Ceramic implant surgery therefore requires good intuitions. While category 1 bone (extremly hard with little blood circulation) must be prepared oversized in order to create cavities for subsequent callus formation, soft bone can be prepared undersized. Once ceramic implants are osseointegrated, the rules for the prosthetic build-up are more sensitive than those for titanium implants. Due to material properties, titan implants show a lower ductility and can therefore better compensate occlusion and articulation particularly in case of slight deflections. In contrast, ceramic implants are securely fixed in the bone and cannot be moved. Solitary ceramic implants should therefore be milled in minimal infraocclusion and without any articulatory contacts.However, this lack of mobility is also a major advantage of ceramic implants. Against university doctrine, one millimeter bone around the implant is no longer necessary for ceramic implants. As long as the ceramic implant is primarily stable, it will heal. This poses the requirement to learn to “think in ceramic”: This simply means that those areas of the implant that are completely surrounded by bone form the actual implant and those areas where periosteum or gingiva is fixed around the implant form the abutment. Since the periosteum and gingiva creepingly attach to the ceramic, completely new methods of ceramic implantology are possible. There is no attached gingiva to titanium or other metal abutments. Therefore, a ceramic abutment is the absolute standard even in usual, titanium-based implantology.
Patient case
In early October 2016, a patient presented with prosthetically and conservatively insufficiently restored adult dentures. A bridge region 34 to 37 (Figs. 7–9) was in especially high need of renewal and the devitalised tooth 37 exhibited apical alterations in the form of radicular cysts (Fig. 10). These teeth were not viable for another prosthetic restoration due to their deficiencies. The apical findings in region 35 and 37 were confirmed by the CBCT, verifying the clinically noticeable pressure pain in region 35 and occlusal pain in region 37. Patient and dentist agreed on immediate implantation with two-piece ceramic implants as an ideal form of socket preservation. Immediate implantation can thus be achieved in spite of chronically apical inflammation.
In cases such as this, the perioperative preparation of the patient is decisive. Two weeks ahead of implantation, the patient’s physiological constitution and metabolism are primed for bone- and soft-tissue regeneration by a selection of nutrients (BHP® according to Dr Nischwitz). The patient’s immune system is optimally prepared. During surgery, the alveolus must be thoroughly cleaned and disinfected, as ceramic implants only become incorporated in healthy bone. For disinfection, ozone is used. Periodontal fibres and any granulation or cystic tissues must be removed completely. The implant can be viewed as the “bonus on top”, supporting the whole alveolus when inserted primarily stable. In this case, the author opted for two-piece ceramic implants in order to prevent any tongue pressure and to allow for absolute rest during healing. This surgical procedure can be standardised, has a high success rate and is both painless and minimally invasive—the results speak for themselves (Figs. 11–14).
Conclusion
Ceramic implants, particularly immediately inserted ones (SCC®—Short Cut Concept according to Dr Karl Ulrich Volz), offer huge advantages over titanium implants. While immediate titanium implants, particularly in the posterior region, are only possible in a few cases, immediate implantation with ceramic implants is possible in almost all cases of tooth extraction. Therefore, immediate implantation with ceramic implants is the gold standard, provided a strictly followed protocol. If both the systemic support of the bone and tissue regeneration are well-functioning, the dentist is working carefully and the alveolus is disinfected properly and precisely examined for isolated osteolysis, ceramic implants are ideal for socket preservation. It then works almost like a plug. Since the alveolus is smaller than the implant, the wounded area, which has to heal, is also smaller. At this stage, endogenic regenerations processes in bone and tissue are working at full power. Particularly with regard to aesthetics, immediately inserting ceramic implants is the ideal time to operate according to the author. With a success rate of over 90 per cent, complicated immediate implants can also be carried out as routine in the posterior region in most cases.
Following this procedure means that the patient does not require an additional implantation appointment, the bone- and soft-tissue are immediately supported and—in addition to the significantly more efficient process for patient and dentist—the immediate implantation is generally completely painless.
contact
Dr Dominik Nischwitz
Specialist in Biological Dentistry
and Ceramic Implants
DNA Health&Aesthetics
Heerweg 26
72070 Tübingen, Germany
Tel.: +49 7071 975977
info@dnaesthetics.de
dnaesthetics.de